|
|
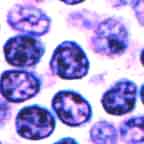
Low Grade Lymphomas
|
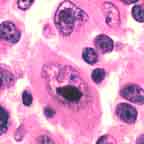
Higher Grade Lymphomas
|
| • The cells are small with clumped chromatin and inconspicuous
nucleoli. The growth pattern may be diffuse (as in small lymphocytic lymphoma)
or follicular. The growth is relatively non-destructive. |
• The cells show large nuclei containing open (clear) or
powdery chromatin. Nucleoli are usually prominent. Some higher grade lymphomas may have moderate amounts
of cytoplasm. Almost always they grow diffusely and destructively. |
| • Patients mostly older, usually 50-60, rarely < 40 y/o. |
• The
median patient age is 60. These lymphomas account for almost a half of adult
lymphomas but are not uncommon in children. |
| • Patients present with multiple painless, enlarged lymph
nodes, uncommonly with significant extranodal extension. Extranodal organs
are only rarely involved except for the bone marrow, which is positive 75% of
the time. |
• Patients often present with a single, quickly growing nodal or
extranodal mass. Focal or extranodal disease is much more common. |
| • Pivileged sites (CNS, testis) are not invaded. |
• Lymphoma may involve privileged sites. |
| • Though not common, spleen and liver involvement takes the
form of many tiny deposits. |
• Though not common, spleen and liver involvement takes the
form of large, destructive masses. |
| • Although significant numbers of lymphoma cells spill into the peripheral
blood only in small lymphocytic lymphoma, numbers of circulating low grade lymphoma cells
can usually be detected by sensitive techniques. |
• Blood involvement with these relatively bulky cells is unusual. |
• In vitro lymphoma cells:
- respond to regulatory molecules
- cannot be transplanted
- will not grow in culture
|
• In vitro lymphoma cells:
- grow autonomously
- can be transplanted to immunodeficient hosts
- subsist indefinitely in culture (immortalized)
|
|
|
It is, however, a paradox of all lymphomas that the indolent, low grade
lymphomas permit long survivals but are virtually uncurable and may not be treated initially. On the
other hand, the higher grade lymphomas are often rapidly deadly, but all
patients are treated and some respond even to the point of complete cure.
Behind this paradox is the observation that both chemotherapy and radiotherapy
target rapidly dividing cells.
For some lymphomas, such as Burkitt's lymphoma, the cell of derivation has not been definitively identified. Other lymphomas start by resembling their cell of origin but
subsequently dedifferentiate.
For example, follicular center cell lymphomas may enter a diffuse growth phase,
belying their origin from cells that grow in follicles. In such cases
their follicular nature must be inferred from softer evidence, such as the
presence of characteristic small-cleaved follicular center cells,
certain antigens such as CD10, or the characteristic t(14;18) BCL-2
gene rearrangement.
Also, many low-grade lymphomas tend to progress to
higher grade disease. In Richter's transformation, for example,
small lymphocytic lymphoma promotes itself to diffuse large cell lymphoma.
Immuno- and Genophenotype:
-
With few exceptions B-cell lymphomas express the pan-B cell antigens: CD19,
CD20, CD22. As B-cells reach their final goal (the plasma cell
stage), paradoxically they tend to lose these markers, and so do their
malignant counterparts. Thus multiple myeloma cells are negative for these
antigens.
-
CD5 and CD43, most frequently found on T-cells,
are detected in small lymphocytic lymphoma and mantle cell lymphoma. Small
lymphocytic lymphoma is also reactive for CD23.
-
CD10 is found in many cases of very different types of lymphomas: follicular center
cell lymphomas, B-cell lymphoblastic lymphomas, and Burkitt's lymphomas.
-
Most follicular lymphomas, especially low grade ones, rearrange
the BCL-2 gene, t(14;18).
-
Most Burkitt's lymphomas rearrange the MYC gene, t(8;14).
-
Most mantle cell lymphomas rearrange the BCL-1 gene, t(11;14).

Table of Contents |
Next section |
Previous section
|